
Collision of Cargo Vessel Nomadic Milde and Bulk Carrier Atlantic Venus1
As part of their normal operations, ships are often at anchor in order to wait for a berth, undergo repairs, bunkering or for some other reason. At anchor, ships are affected by external forces, the type and weight of the anchor, the nature of the sea bottom, the holding power of the anchor and other factors. This can result in a ship at anchorage dragging the anchor, which can result in grounding or a collision. These accidents can cause serious structural damage to the ship as well as damage to the marine environment.
This report includes an example of an accident caused by dragging anchor and an examination of possible ways to prevent a ship from dragging its anchors.
Summary
At 16:55 local time on May 8, 2020, the cargo vessel Nomadic Milde, which was anchored in the Mississippi River near New Orleans, Louisiana, began to swing due to the strong current of 4 to 5 knots. This ship dragged its anchors and eventually collided with the bulk carrier Atlantic Venus, which was anchored nearby. After colliding with the Atlantic Venus, the Nomadic Milde struck a nearby chemical dock and then grounded on the bank. There were no injuries but the Nomadic Milde released an estimated 50 liters of lube oil into the river. Damage to the two ships and the dock was an estimated $16.9 million.

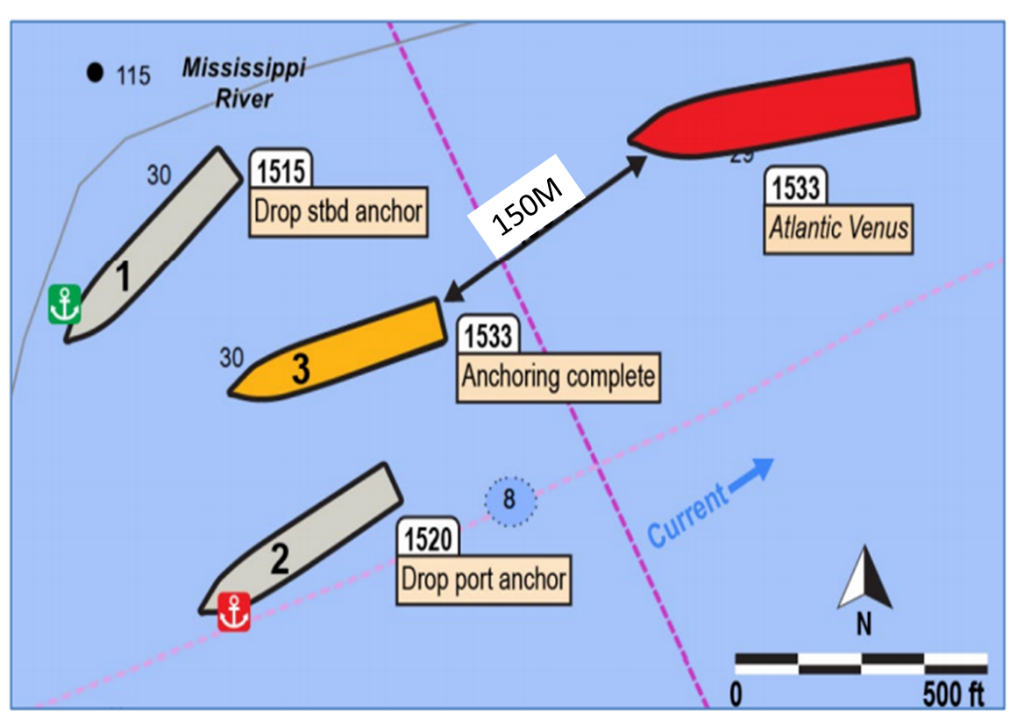
Figure 12: AIS symbols of the vessels anchored at 1533 on May 8 (Source: PortVision, annotated by NTSB).
Vessel Data
Nomadic Milde
Length 138.1m, 9,530 tons, draft 8.05m, Marshall Islands registry, 670hp bow thruster, crew of 16
Anchor: Stockless anchor (637kN)
Atlantic Venus
Length 179.9m, 21,441 tons, draft 6.4m, Panama registry, crew of 20
Accident Timeline
On May 8, the Nomadic Milde completed loading lead concentrate at a facility 8 miles from the location of the accident.
1320: A pilot boarded the ship for the transit to an anchorage where the vessel was to undergo a repair the following morning.
1350: The Nomadic Milde began the transit to the anchorage under the direction of the pilot.
The pilot showed the master and chief officer the intended anchoring position on the ship’s electronic chart and information display system (ECDIS). The pilot informed the master of his plan to let go the starboard anchor first and then the port anchor in order to establish a “good spread” between the two anchor chains. The reason was the forecast for strong and gusty wind in this area in the afternoon.
1515: At the anchorage, the pilot positioned the Nomadic Milde between two bulk carriers in ballast and, with a heading of 228 degrees, requested the starboard anchor let go. (water depth is about 15 meters).
1520: The port anchor was let go when the vessel was on a heading of 242 degrees.
The starboard anchor was heaved to 4 shackles (110 meters) on deck and the port to 3 shackles (82 meters) in the water.

Figure 2: Nomadic Milde positions from VDR.
The green anchor icon indicates the starboard anchor drop position, and the red anchor icon indicates the port anchor drop position.
Scale approximate. (Background source: NOAA ENC 6LA54M)
1532: The pilot informed the master that the anchoring was “all finished” and that “[the ship] looks good.” The pilot also cautioned that there was “considerable current” and that it would be “a good idea to keep the engine on a short standby” and “to keep a short leash on [the ship].”
The bulk carrier Atlantic Venus was down river with its bow about 150 meters from the stern of the Nomadic Milde.
1533: The Nomadic Milde continued to shift position and heading.
1540: The pilot departed the bridge and subsequently left the ship.
The second officer on watch on the bridge activated the anchor watch alarm on the ECDIS and set it for a maximum radius of 180 meters. The radius was based on the length of the ship and the amount of anchor chains. However, after the accident, the second officer said he did not remember the basis for the 180 meter setting.

Figure 3: Nomadic Milde’s initial movements from 1533 to 1547 from the vessel’s VDR, scale approximate. (Background source: NOAA ENC 6LA54M)
1557: The Nomadic Milde continued horsing motion, moving at about 1.8 knots over ground, and was 107 meters off the starboard bow of the Atlantic Venus.
1602: The chief officer and second officer began the anchor watch handover.
The chief officer, who was unfamiliar with the ship’s ECDIS system, asked the second officer why the ship was not in the middle of the ECDIS anchor watch circle. The second officer offered to assist the chief officer with the ECDIS, but they did not further discuss the ship’s position at anchor.
1613: The officer on watch aboard the Atlantic Venus called the Nomadic Milde over VHF radio to ask that they monitor their holding position.
1639: The chief officer of the Nomadic Milde said “we are too close” and asked the second officer what the distance was to the Atlantic Venus. From the portside radar, the second officer replied that the distance was “point zero three cables” (55 meters).
1640: The chief officer asked to have the chief engineer call him on the bridge (and then have the engine ready).
1641: The master of the Atlantic Venus radioed the Nomadic Milde to say that both vessels were very close and in an unsafe condition.
1642: The chief officer on the Nomadic Milde informed the master that they were too close to the ship behind them. The master immediately went to the bridge. At that time, the distance between the stern of the Nomadic Milde and the bow of the Atlantic Venus was 45 meters.
1645: The Nomadic Milde master contacted New Orleans VTS and said he needed a pilot to “change position.” VTS told him to contact his agent to arrange for a pilot.
1647: VTS told the Nomadic Milde that it appears that the ship is dragging anchor or maneuvering. VTS said “make sure you do not raise your anchors…maneuver with your engines to stay safe but do not leave your present location…wait for a pilot.”
1649: The Nomadic Milde’s master called the ship’s agent and asked for a pilot. The agent informed the master that this would require 2 to 3 hours.
To reduce the swing of the ship, the master began using full ahead engine, along with the bow thruster and rudder.
1655: The port side of the Nomadic Milde collided with the bulbous bow and anchor chains of the Atlantic Venus.
1725: The first assist tug arrived to hold the Monadic Milde in position. Thirty minutes later, two pilots arrived and boarded the Nomadic Milde and Atlantic Venus.
1856: The speed of the Nomadic Milde increased ahead toward the shore. The pilot responded by using the ship’s engine and rudder in several ways.
1858: The bow of the Nomadic Milde struck the shore at a speed of 6 knots and then grounded.

Figure 4: GPS positions from the time the Nomadic Milde’s starboard anchor was let go at 1515 to the collision with the Atlantic Venus at 1655. Note: the GPS receiver is located on the main mast above the bridge of the Nomadic Milde. Scale approximate. (Background source: NOAA ENC 6LA54M)
Analysis (NTSB)
1) Dragging anchor
The position and heading of the Nomadic Milde were unstable from the time the ship arrived at and anchorage. The ship moved about 220 meters toward the shore from the position where the starboard anchor was let go (1546). This was twice the length of the extended starboard anchor chain, which indicates that this anchor may be dragging. The first six minutes of anchor dragging (1539 to 1545) started within 10 minutes of when the pilot told the master (1532) that the anchoring was “all finished.”
The pilot left the ship while the ship was still moving (1540).
If the bridge team and the master had realized that the ship was dragging anchor or were worried about this possibility before the pilot left the ship, they might have been able to ask the pilot to remain on board to deal with this problem.
2) ECDIS
The second and chief officers both stated that the ECDIS is a method for monitoring the anchorage position of the Nomadic Milde. In particular, in areas where there is risk involving hazardous objects, the weather or currents, the ECDIS must be used as a method for monitoring a ship while it is anchored with regard to continuous caution about the status of the ship and if the ship is dragging the anchors.
The second officer activated the ECDIS anchor watch alarm and the alarm should have sounded if the ship moved beyond the radius that was input. Both the second and chief officers do not remember if the anchor drag alarm was activated. Initially, there was an estimated distance of 150 meters between the stern of the Nomadic Milde and the bow of the Atlantic Venus. The anchor drag monitor alarm setting of 180 meters was therefore too large and made it impossible to receive a timely warning of anchor drag. (Author’s note: The NTSB report does not state where the center of the anchor drag monitoring radius was.)
Between 1551 and 1557, the Nomadic Milde started to swing to starboard and moved about 244 meters during approximately six minutes while dragging the anchors.
When the chief officer took over the watch from the second officer, the chief officer realized that the ship was not in the center of the anchor watch circle. However, he did not ask if the ship had dragged the anchors or if the ship was firmly in place at the anchorage site.
3) Monitoring of the ship’s position
When the chief officer took over and saw that the ship was not in the center of the anchor watch circle, he did not cross-check the ship’s position. Even after the Atlantic Venus sent the first warning about monitoring the ship’s position, the chief officer did nothing to follow-up on this concern.
There was no evidence indicating whether or not the officer on watch had used any method other than the ECDIS anchor watch alarm to check the ship’s location. The ship’s radar supplies information for cross-checking if the distance to another ship or object has decreased or if a ship at anchor has moved.
There was adequate evidence to warn the bridge team that the Nomadic Milde was definitely not anchored. If this evidence had been used, the master would probably have become worried about the situation sooner. Furthermore, there probably would have been enough time to take the actions needed to deal with this problem.
4) New Orleans Vessel Traffic Service (VTS)
The master contacted VTS and the agent to ask for a pilot but was told he would have to wait a few hours. VTS told the master to not raise the anchors and maneuver using the engines. The master followed these instructions. However, leaving the anchors severely restricted the bridge team’s ability to control the ship in the strong river current even when using the main engine full ahead along with the bow thruster and rudder.
Probable cause (NTSB)
The NTSB concluded that the bridge team of the Nomadic Milde did not effectively monitor the ship’s position. As a result, the bridge team did not notice that the ship was moving toward another nearby ship by moving from the original anchorage position due to dragging anchors and the strong river current.
Examination/Analysis
As is explained below, there were many unsafe conditions and unsafe activities associated with this accident. One of these items or a chain of these safety problems caused the accident. Preventing an accident caused by anchor dragging requires an awareness of unsafe conditions and activities and making improvements before these issues create a problem, if possible.
1) Selection of the anchorage
While anchored, the Nomadic Milde was exposed to a strong river current (4 to 5 knots) and strong winds were forecast later in the day. Therefore, there are questions regarding the selection of an anchorage with ships very close on both sides. In these conditions, the Nomadic Milde was anchored only 150 meters from the ship behind it. This cannot be called good seamanship.
2) Method used for anchoring the ship
Holding the ship in place with two anchors (using both the port and starboard anchors) was selected as the method to anchor the Nomadic Milde in the steady river current and conditions with strong wind expected. This may be the standard method used in this location. However, with starboard anchor heaved to 4 shackles (110 meters) on deck and the port to 3 shackles (82 meters) in the water, there was not enough holding power to prevent the ship from moving.
Normally, there is an angle of 120 degrees between the two anchor chains when two anchors are used. This is said to result in the same proof of load as when using a single anchor. Although Figure 2 does not show an accurate figure for this angle, it was probably close to 120 degrees. Consequently, the holding power of the anchorage was about the same as with a single anchor (637 kilonewtons). When a ship is expected to swing back and forth, this is not sufficient strength to withstand the forces of the current and wind on one side of the ship.
3) Bridge team management (BTM)
The chief officer was not familiar with the ECDIS and asked the second officer why the ship was not in the center of the anchor watch circle. However, the chief officer then said nothing more about this subject without having received a sufficient reply.
This violates a basic guideline of BTM because a concern of one crew member must be checked by a discussion of everyone present.
Furthermore, the pilot said “[the ship] looks good.” at the anchorage and he left the ship either immediately before anchor dragging started or as dragging was occurring. At that time, the master and chief officer had a duty to confirm the ship’s status themselves instead of relying solely on the pilot’s statement. In addition, the bridge team needed to confirm the condition of the anchorage, any movement of the ship, the status of the anchor chains and other items. If they had any doubts, they should have asked the pilot for assistance.
Consequently, we can conclude that bridge team management by the individuals on the bridge, including the pilot, was deficient.
4) The Anchor Watch (monitoring, responses, etc.)
During this incident, the anchor watch did not respond to problems sufficiently. Anchor watch includes the following tasks.
- Fixing the position where the anchors are let go and determination of the circle for swinging of the shipConfirmation of the position of the anchors (anchor dragging detection)
- Confirm the ship’s position periodically by using several methods, including a visual check and confirm that the ship is within the designated circle.
- Check conditions near the ship (ships and other obstacles)
- Watch for changes in the weather and sea conditions
If anchor dragging is suspected, there is a ship nearby, a sudden change in the weather or sea conditions that affects the anchorage, or some other event, the master must be notified immediately and then actions must be taken as needed.
ECDIS is the current method used to check for a dragging anchor, as was the case with this accident. Although the ECDIS can be used to confirm that the anchor is dragging, this capability of the ECDIS was unfortunately not sufficiently used by the Nomadic Milde bridge team.
Even when the ECDIS is used, the circle for the ship’s swinging circle must be accurately determined and information must entered in the ECDIS accordingly.
(Note: In this report, it is not clear where the center of this circle was. Furthermore, the second officer set 180 meters as the swing (anchor watch alarm) radius but was unable to provide an accurate response concerning the basis for selecting this radius.)
The following is a simplified explanation of the preparation of a swinging circle for a ship anchored with a single anchor3.
Step 1: Enter the position where the anchor was let go (based on the positon of the bridge) and the heading of the ship’s bow.
Step 2: Confirm the position of where the anchor was let go by adjusting for the distance between the location used for the measurement (the bridge) and the ship’s bow.
Step 3: Draw a circle (radius is the sum of the length of anchor chain released and the length of the ship) centered on the anchor position.

Figure 5: Determination of the swinging circle of the ship
If the ship goes outside this circle, the ship may be dragging the anchor.
Since ships started using the ECDIS, the monitoring of anchor dragging uses the Anchor Watch function (the name may differ depending on the model of the ECDIS used). This makes it possible to set an anchor watch circle in the ECDIS. Even when this function is used, the bridge team must obviously perform visual, radar and other checks periodically to confirm the ship’s position.

Figure 6: Example of an anchor watch circle on an ECDIS (JRC)
5) Actions taken when dragging the anchor
If a ship starts to drag the anchor or anchors, all methods available must be used to stop this problem. First, the anchor or anchors must be raised immediately. When this step is taken, attention must be paid to the following points.
- The capacity of the windlass may be insufficient due to external forces. If this happens, an excessive amount of actions taken may place a burden on the windlass that results in damage and the inability to operate the windlass any longer. (Example: Grounding of Ship A on October 20, 2004, Fushiki Toyama Harbor)
- Use the main engine. The engine can be used to reduce drift caused by the wind or to reduce the effect of external forces in order to raise the anchors more easily. The engine is most effective method to use when raising the anchor. However, caution is required because an excessive load on the engine for a long time can damage the engine, such as by increasing the temperature of the exhaust. (Example: Grounding of Ship B on October 6, 2006, Kashima Harbor)
- Another possible action is the use of the anchor on the other side of the ship. In some cases, letting go the other anchor will reduce dragging. Furthermore, the bridge team must ask someone to send one or more tugboats. However, the availability of tugboats may be limited during inclement weather.
- Slipping the anchor4
It may be impossible to raise the anchor because of external forces or damage to the windlass. This could prevent the ship from moving to avoid an imminent danger or could pose a risk to the environment. If this situation, the master must consider cutting the anchor loose to enable the ship to begin moving.
To slip the anchor, normally the bitter end (the end part of the anchor chain that remains inboard when a ship is at anchor) is cut. This is why ships must always have a quick release device readily available for cutting the anchor chain. In addition, crew members must be trained in the use of this device so that the anchor can be cut loose quickly in the event of an emergency.
Figure 7 shows how the anchor can be easily cut loose on the ship. As shown, the bitter end can be easily cut loose from the chain locker (quick release).

Figure 7: Quick release and bitter end
To cut loose the bitter end, a hammer is used to remove the pin by knocking the red section of the quick release pin to the left. (Figure 8)
For additional information about this subject, Figures 9 and 10 show the structure of the quick release section and the bitter end.

Figure 8: The anchor chain quick release mechanism (inside the bosun’s store)

Figure 9: The quick release mechanism and bitter end_1 (With the pin is in the normal position)

Figure 10: The quick release mechanism and bitter end_2 (With the pin moved to the left)
As this report has explained, dragging anchor is a problem that can occur when navigating a ship. If the bridge team does not respond correctly, dragging the anchor can result in a serious accident. Therefore, the following points must be considered before anchoring a ship. Relevant information must be shared with all parties involved in advance (a preliminary briefing required).
- Confirm the conditions at the planned location for anchoring the ship (condition of the bottom, depth, weather and sea conditions, nearby obstacles, and other items).
- Determine the method for anchoring the ship (releasing the anchor).
- Calculate external forces and the holding power of the anchor and confirm the limitation of external forces for anchoring.
- Confirm the system for monitoring anchor dragging and the equipment used for this monitoring.
Decide the internal for confirming the ship’s position.
If an ECDIS system is used, familiarize with how to use the ECDIS
Set the anchor swinging circle
Activate the warning alarm
- Responses to anchor dragging (explained earlier)
-----------------------------------------------------------
References
1NTSB Accident Report MAB-21-15
Collision of Cargo Vessel Nomadic Milde and Bulk Carrier Atlantic Venus
2Figures 1 through 4 were prepared by the author using figures in the above NTSB Accident Report
3Prepared using as reference P210 of Practical Navigator (Seizando Shoten Publishing, Hiroshi Sekine editor)
4Prepared using as reference P215-216 of Practical Navigator (Seizando Shoten Publishing, Hiroshi Sekine, editor)
Related news
-

Ask an Expert: Cyber risk management
25/06/2025
-

Ask an Expert: Sustainable Ship Recycling
24/06/2025
-

Risk Focus: Vessel cyber security
25/06/2025
-
